Dr. Daniel A. Medalie in Cleveland, Ohio is an internationally recognized expert in the field of Female to Male gender affirmation chest or "top" surgery. He has been practicing since 1999 and has performed well over 3000 gender affirmation chest procedures. He has also published multiple articles and lectured extensively in the field of chest masculinization. He has been featured in several documentaries about transgender surgery including ones on MTV and LOGO tv. He also focuses on top surgery revisions and is happy to provide free virtual consultations for patients desiring another opinion or revisions of their previous top surgery.
IMPORTANT TOP SURGERY FAQs AND POST-OP INSTRUCTIONS ARE AT THE BOTTOM OF THIS PAGE-PLEASE SCROLL DOWN
*Plastic surgery results can vary.
What people are saying about Dr. Medalie on Google:
I'm a physician that specializes in the care of transgender people. I have seen hundreds of top surgery results over the years. Maybe even 1,000.
Dr. Medalie routinely produces the best results I see on any of my patients that get top surgery done. The worst outcome top surgery I have ever seen done by him was a 9/10. The best I've seen done locally in michigan I'd call an 8/10. Literally, the worst results I've seen on anyone done by this guy are better than the best results done by everyone else. Some of these patients come back and you can't even tell that they ever had top surgery done. I don't even know how he does the micro suturing or whatever it is that he does to not leave the telltale 1/2cm thick double incision scar lines but the results are amazing.
I have never talked to Dr. Medalie personally. I don't know him personally in any capacity or have any vested interest in his clinic or his success. This is my real honest opinion after eight years of treating transgender patients and seeing the results of the work of many surgeons.
Unequivocally he is my top recommendation for top surgery. It's not even close.



Dr. Medalie explains the various options for FtM Gender Affirmation Top Surgery
Dr. Medalie performs FtM Double Incision Mastectomy and Nipple Grafting
Dr. Medalie Performs FtM Peri-Areolar Mastectomy with circum-areolar mastopexy

Dr. Medalie reviews his FtM top surgery results comparing the Peri to DI technique
FTM Top Surgery Peri-Areolar Technique vs. Double Incision with Nipple Grafts
| Aspect | FTM Top Surgery – Double Incision | FTM Top Surgery – Peri-Areolar |
|---|---|---|
| Definition | Chest masculinization procedure that removes breast tissue and excess skin through two horizontal incisions across the chest, with nipple-areola grafting or resizing. | Chest masculinization procedure performed through circular incisions around the areola, removing breast tissue with minimal skin excision. Can be partial (7-11 o'clock) or circumferential around the areola |
| Ideal Candidates | Trans men or non-binary individuals with medium-to-large chest size, excess skin, or reduced skin elasticity. | Best for small chest sizes (A–small B cup), minimal excess skin, and good skin elasticity. |
| Surgical Technique | Two incisions along the lower chest; breast tissue and skin removed; nipples resized and grafted in masculine position. Liposuction of central and lateral chest and pre-axilla. | Partial or concentric incisions around the areola; breast tissue removed; areola may be reduced; skin tightens naturally over time. Liposuction of pre-axilla |
| Scarring | Moderate to significant scars across the chest wall (fade over time but permanent). I try and place them in the shadow of the pectoralis muscle | Minimal scarring limited to the edge of the areola, often less visible. Can widen over time if circum-areolar |
| Nipple Sensation | Higher risk of loss of sensation due to free nipple grafting. | Greater chance of preserved nipple sensation since nipple is usually left attached. |
| Anesthesia & Surgery Time | General anesthesia; approx. 1.5-2 hours. | General anesthesia; approx. 2–2.5 hours. |
| Recovery Time | 4–6 weeks for most physical activity; no heavy lifting for 8 weeks, compression garments required for 2 weeks. | 4-6 weeks for most physical activity; no heavy lifting for 8 weeks, compression garments required for 2 weeks. |
| Risks & Complications | Bleeding, infection, nipple graft failure, contour irregularities, hypertrophic scarring. | Risk of skin wrinkling, nipple stretching, under-correction, or need for revision if excess skin remains. |
| Longevity of Results | Permanent, with possible revisions for scars or contour refinements. | Long-lasting, but higher chance of revision surgery if chest skin does not retract as expected. |
| Cosmetic Outcome | Creates a flat, masculine chest even with larger breast size, but with visible scars. | More natural-looking chest with minimal scarring; best cosmetic results only in small-chested patients. |
 Summary:
Summary:

When considering FTM top surgery, the choice between the double incision technique and the peri-areolar technique depends on chest size, skin elasticity, and desired outcomes. The double incision method is most effective for medium to large chests, providing a flat, masculine contour with permanent results, though it leaves visible chest scars and will almost certainly reduce nipple sensation. The peri-areolar approach, on the other hand, is best suited for individuals with smaller chests and good skin elasticity, offering subtle results with minimal scarring and a greater chance of preserved nipple sensation (but still variable). Both procedures significantly reduce gender dysphoria, improve self-confidence, and help trans men and non-binary individuals feel more comfortable in their bodies. Dr. Medalie is a world expert in gender affirmation top surgery and has been performing the procedure for over 25 years. He provides free virtual consults to prospective patients both for primary top surgery and revisionary top surgery.
Gender Affirmation Top Surgery- The Peri-Areolar Technique
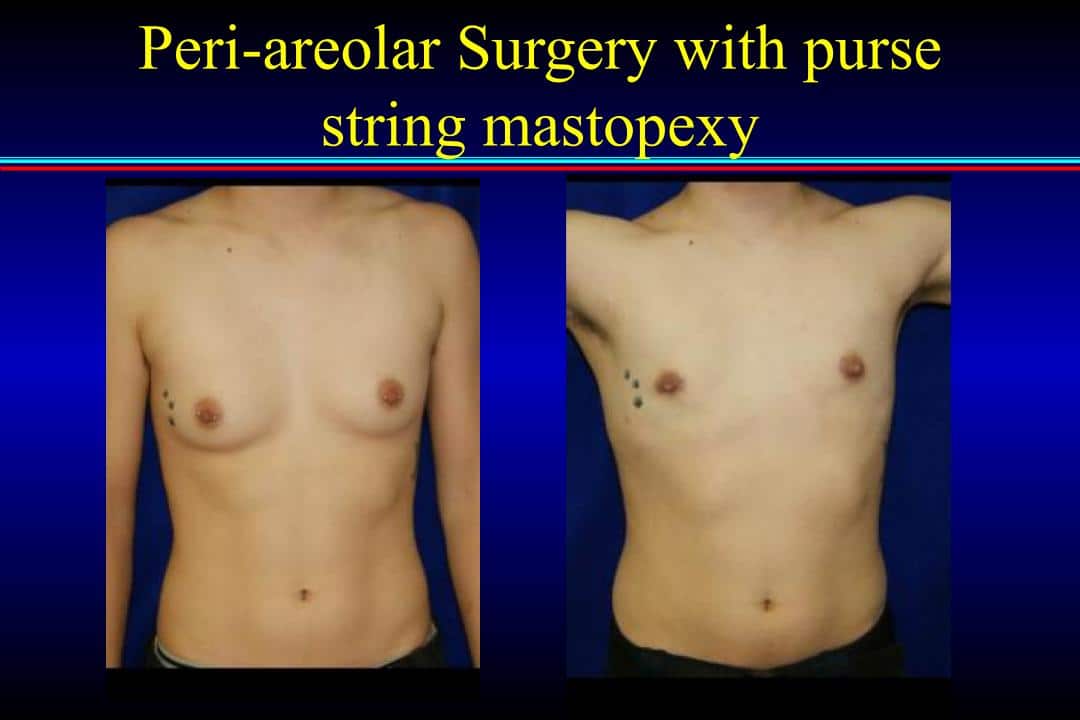
In general, patients who have smaller breasts can have the entire surgery performed by having a small incision at the outer edge of the areola from 11:00 to 7:00 o’clock. A lighted retractor and surgical scissors are used to perform a complete sub-cutaneous mastectomy. Liposuction of the chest is also performed as needed (typically in the pre-axillary fat pad).This provides the most optimal results and can be almost invisible after it heals. If the skin appears a little looser at the start of the case then a complete peri-areolar incision is made. A small amount of skin is removed (in a doughnut pattern , also known as-“peri-areolar or “purse-string” mastopexy”). A subcutaneous mastectomy is performed and then the outer edge of the skin is closed with a purse-string to the newly down-sized areola. By necessity, the edges of the incision around the nipple will be “scalloped” or bunched up initially. This settles down to a great degree over time. If the patient understands that scar revision may be necessary, this is a very reasonable approach. It is more complicated however and takes longer in the OR. The nipple may also experience compromise of its blood supply and also have sensation or erectile capacity changes. More information and a step by step guide to the peri-areolar top surgery procedure can be seen on my peri specific page. Click HERE to check it out. Excellent peri results can be seen in multiple patient photos in my Top Surgery Gallery
Gender Affirmation Top Surgery- The Double Incision Technique
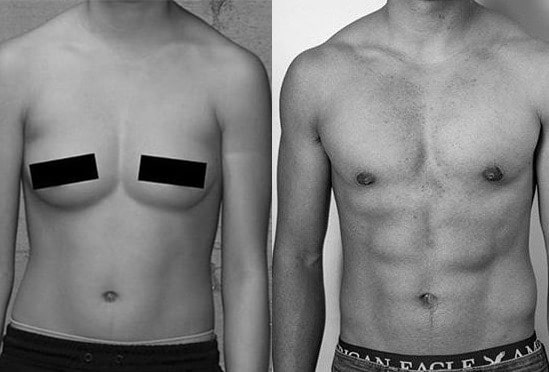
In those patients with a large amount of breast tissue with excessive skin of poor quality and droop, it is usually recommend to remove the excess skin and breast tissue in the crease of the pectoralis muscles (elliptical or double incision mastectomy) and put the nipples and areolae back on as grafts. This surgery has the advantage of immediate and predictable results. I can contour the skin flaps and place the nipples where I want to. It has the disadvantage of permanently altering the sensation and erectile capacity of the nipples (and sometimes the pigmentation), and it leaves larger scars on the chest. Over time they fade and flatten out. At each end of the scar, “dog-ears” may form. These are small bunches of tissue created by the closing of the ellipse as a straight line. They tend to settle down over time, but may need to be revised. I always try and address the dog ears at the time of surgery but this may extend the length of the scar. Dog ears are more likely in patients who are heavier and have more tissue to start with. I always perform liposuction of the central and lateral chest (to flatten the dog ears) as well as the area in front of the armpit (pre-axillary fat pad). I have been asked why a scar may meet in the center of the chest on some top surgery results but not on others. This is dependent on pre-existing anatomy. If the tissue meets in the middle (such as in the example right below) then the scar by necessity will meet in the middle (this can’t be seen in the example because of the patient’s chest hair.) In general my goal with the DI is to leave a scar that is straight in the midline and then angles up laterally on the edge of the pectoralis major muscle. If the patient subsequently works out the chest muscle, over time, the scar will be hidden in the shadow of the muscle. More information and a step by step guide to the double incision top surgery procedure can be seen on my DI specific page. Click HERE to check it out. Many excellent patient DI before and after results can be seen in my Top Surgery Gallery

FTM Top Surgery Revisions
I get contacted by many patients who have had FtM top surgery and are now seeking a revision of their chest. If they are my own patients seeking revision, the problems are almost always small and can be taken care of under local anesthesia in my clinic (touch up liposuction or dog ear revision). Usually when I am contacted by a patient who has had a procedure by another physician, the results are quite poor (because otherwise the patient would have gone back to his original surgeon), and the patient needs to go back to the OR for a successful outcome. Please click HERE to go to my dedicated revision page and find out more information about FtM top surgery revisions. I would be happy to review any before and after photos a prospective patient wishes to send me, and I will do my best to give an idea of what might be necessary to improve the cosmetic outcome.
FTM Top Surgery Scarring
Many patients ask about what the scars will look like (especially for the double incision surgery DI). The patient below posted these himself on Transbucket. He shows how his scars have evolved from 1 week after top surgery to 1 month, to 3 months and finally to 2 years post mastectomy. The scars which are quite visible initially fade over time and fall into the line of the pectoralis major muscle of the chest. This is an important point because many patients are afraid of the DI because of how the scars look. I think that the DI can give a better result with better contouring of the chest and nipple position than a peri-areolar procedure in the right patient. That does not mean that it is the best choice for all people and this is an important conversation that I have with all of my top surgery patients. But it should reassure prospective surgery patients that very good results are possible with DI surgery.

Scheduling Top Surgery
If you are local to the Cleveland area within 60 minutes of our office, I want to see you in the office for an in-person consultation. Please call our office to set up an appointment. You will need clearance letters from mental health providers in order to schedule surgery. Please see below for information regarding the therapist letters.
I frequently perform operations on FtM patients who live out of town and are unable to easily to see me in consultation prior to the procedure. I have several requirements for these patients (all of these must be fulfilled prior to scheduling):
- I must have a clearance letter from a therapist that you have seen for at least 1 year. If you haven’t seen a therapist for at least 1 year, you will need two clearance letters for surgery. One letter needs to be with a mental health provider that you have seen for at least 6 months. The other letter can be a 1 time assessment with a different mental health provider confirming the diagnosis of gender dysphoria. One of the mental health providers needs to have a degree of PhD or MD (psychologist or psychiatrist). The letters must adhere to WPATH standards and state that you have been diagnosed with gender dysphoria and are a good candidate mastectomy surgery. The letters need to state that you understand the surgery is irreversible and life-changing. This must be sent to us (e-mail, fax or mail) before we schedule the surgery.
- I must see pictures prior to scheduling surgery (front and side with arms down). Please do not hold the camera yourself.
- Patients need to download a history form (please click on link), fill it out, and send it to my patient care manager, Valerie.
- We are no longer accepting insurance for any type of transgender surgery. We do provide a letter with all surgery codes to help you get reimbursed by your insurance company for your top surgery.
- Dr. Medalie booking about 1 – 2 months out for surgery.
Typically I will perform a phone consultation several weeks prior to the procedure. I will then perform the operation and see the patient back in my clinic in 5-7 days to remove drains and change the dressing. This means that the patient will spend around 1 week in the Cleveland, Ohio area. Patients who live far away, but can drive to Cleveland (1-6 hrs.), can go home the next day and drive back to see me for their first post-operative appointment. I will then follow the progress of the patient via e-mailed pictures. Occasionally, I have had patients who have gone home and had their primary care doctor remove the drains and perform the first dressing change. I do not prefer this but do allow it if the patient can assure me of good care. My patient care manager has information about hotels in the area as well as financing. For all logistical details she is the best person to contact. Her e-mail is valerie@clevelandplasticsurgery.com.
Insurance Coverage and Fees (This is important!)
We do not accept insurance for any transgender surgeries. We will however give you a pre-determination letter with the standard surgical codes that you may send to your insurance company and ask for a reimbursement. Sometimes insurance will cover the facility fee at the Brainard surgery center where I work if they accept the pre-D letters. The codes for the surgery will be simple mastectomy and nipple reconstruction (CPT 19303 x 2, 19350 x 2) and the diagnosis code will be gender dysphoria (ICD-10-F64.9).
Other Procedures for FtM Patients-Liposuction, Body Contouring
Many patients ask whether other procedures can be performed concurrently with the top surgery. The most common procedure asked about is liposuction of the flanks, hips, abdomen and thighs. I do this frequently to help contour the whole trunk and would be happy to discuss this with any prospective patient. Please include the whole trunk (front and back) in the photos sent to me so that I can effectively evaluate you. The cost is variable and depends on the extent of extra liposuction performed and the anticipated time that it will take. To see some of my typical results for liposuction and body contouring, please Click Here.
Below is a patient who requested top surgery and body contouring. Because of the loose skin of his chest he was only a god candidate for the double incision procedure with nipple grafting. In regards to his torso, I felt that with liposuction alone he would have a reasonable result but possibly some retained skin laxity in the lower abdomen. He thus elected to have a lower abdominoplasty in conjunction with his liposuction procedure. This enabled me to tighten his loose skin after aggressive body contouring with power assisted liposuction. He has also been engaged in extensive physical conditioning since the surgery!


Metoidioplasty Surgery






In this operation, the surrounding skin of the clitoris is removed and it is released from the pubis to give the appearance of more length. The glands will appear circumcised in most patients. The final result is a normal appearing, but very small, penis. Actual result will depend on various factors as described below. The outcome is largely dependent upon how much enlargement of the clitoris has occurred with Testosterone. The best results from the metoidioplasty are in patients who are near their ideal body weight and do not have an overhanging mons pubis. In most patients, removal of some skin and liposuction of the fat of the mons will also improve the result. The principal advantage of the metoidioplasty is that it is noninvasive, maintains the sensitivity of the clitoris, and does not create apparent surgical scars. Furthermore, it does not prevent future genital surgery from being done at a later time should one decide. The penis will not, however, appear adult in size, and it is not large enough for vaginal intercourse. Dr. Medalie does not perform urethral lengthening with metoidioplasty. Dr. Medalie typically performs simple metoidioplasty as an outpatient procedure. If a patient desires scrotal construction from the labia majora and insertion of testicular implants, this procedure can be done simultaneously with the non-urethral metoidioplasty.
FtM Top Surgery FAQ
Yes-Both the peri and Di procedures needs to be performed with the patient asleep.
A typical Di takes around 1.5 to 2 hours and a typical Peri last around 2-2.5 hours
I typically give my patients antibiotics on the day of surgery. Post operative infections are rare and are typically related to the dissolving sutures which can sometimes irritate the skin. Please be aware that smoking is the number one reason for post-operative infections and healing problems. I thus require my patients to STOP SMOKING at least 3 months prior to top surgery procedures.
During the surgery, local anesthetic is injected into the tissue using a tumescent technique-this blocks the sensation and also constricts blood vessels. As a result, there is very little bleeding during the surgery. I have NEVER had a patient have a severe bleeding complication post-op, but it is not impossible and a return trip to the OR may be necessary. No one has ever needed a blood transfusion for this procedure. Sometimes a patient will get a little bit of bleeding in the chest and not know it because of all of the dressings. This is called a hematoma and can be addressed under local in my clinic without a return to the OR.
These are fairly well tolerated operations. Pain that may require narcotic pain medicine typically lasts 3-4 days. After that, ibuprofen (Motrin and Advil) is sufficient. I recommend that patients take at least 1 week off from work or school and driving. The post-op care involves a compression vest for 2 weeks and scar massage after that.No heavy lifting is allowed for 8 weeks Most of the swelling and all of the buried stitches have disappeared by 3-4 months.
I recommend that patients refrain from exercise for at least 3 weeks after surgery. Even after 3 weeks, the incisions may be sensitive and patients need to use caution. Full activity including heavy lifting can not resume until the patient is 2 months out from surgery.
Some of the deep sutures under the skin can take up to three months to completely dissolve. For this reason, some patients may report sensitivity issues such as itching for up to three months post-op. Nipple and chest sensation may always be a little numb. Typically my patients have resumed full activity by 2-3 months. The final result including fading of the top surgery scars can take up to 1 year.
Yes – I frequently perform multiple procedures on top surgery patients. Liposuction and tummy tucks are the most common simultaneous surgeries.
The cost of top surgery varies based on:
- Surgical technique required (peri-areolar vs. DI)
- Duration of the procedure
When you consult with Dr. Medalie he will explain your options and e-mail you a comprehensive price quote the same day that includes the top surgery, the anesthesia and the facility costs.
For many more Top Surgery Before and After Photos please check out my gallery by clicking here!
For more, I recommend that you visit TRANSBUCKET.COM. You will need to create an account (but it is free). At this site many of my patients have posted their own photos without my input. This is the best way to see true top surgery before and after photos. I also recommend searching for me on Youtube and Instagram.